All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the MPN Advocates Network.
The MPN Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the MPN Hub cannot guarantee the accuracy of translated content. The MPN Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The MPN Hub is an independent medical education platform, sponsored by GSK, Novartis, AOP, Sobi and Takeda and supported through independent educational grants from Bristol Myers Squibb, Blueprint, Incyte and Merck Sharp & Dohme LLC, Rahway, NJ, USA. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View MPN content recommended for you
Management of MF-related anemia: Current international guidelines
Do you know... According to the NCCN 2026 guidelines for MPN, which therapy is listed as a preferred regimen for patients with MF-associated anemia and ongoing symptomatic splenomegaly and/or constitutional symptoms?
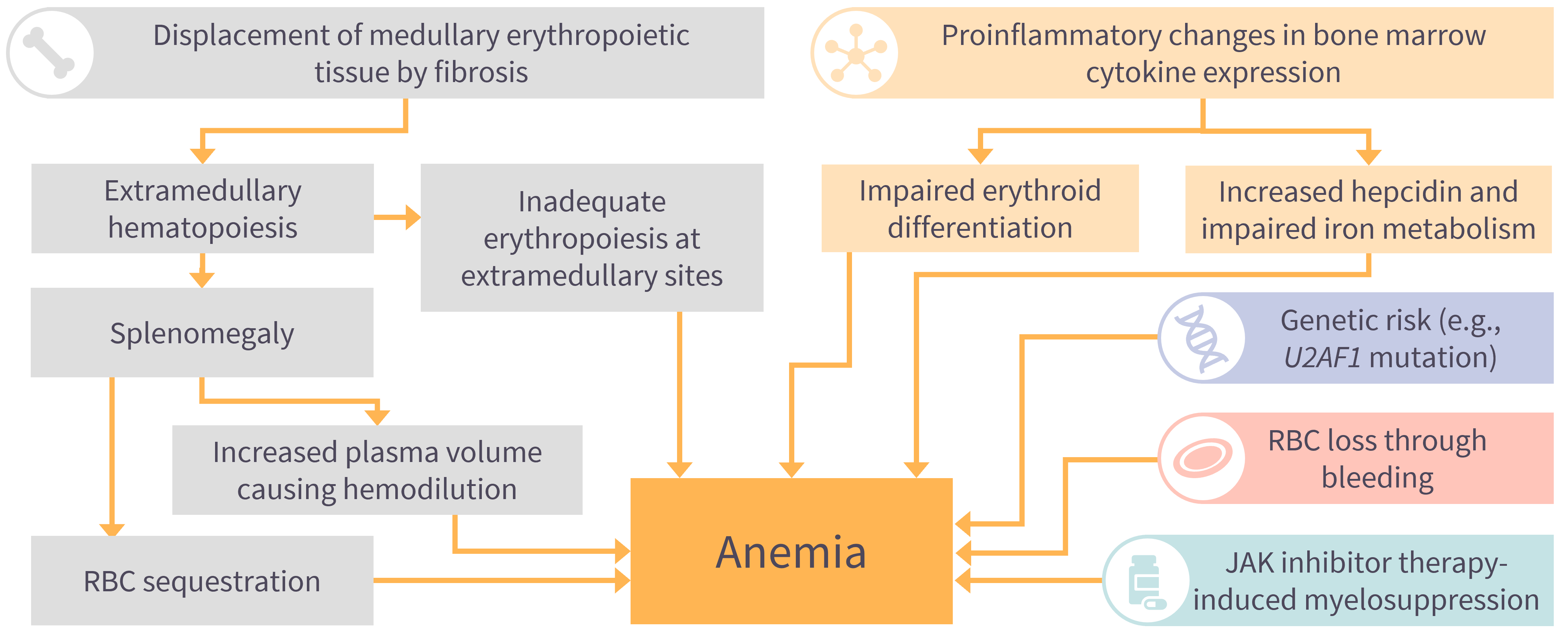
Anemia is one of the most common and clinically significant manifestations of myelofibrosis (MF), with >50% of patients experiencing symptomatic anemia at diagnosis and up to two‑thirds of patients affected over the disease course.1,2 Anemia contributes substantially to symptom burden, transfusion dependence, impaired quality of life, and adverse prognosis, and it frequently complicates therapeutic decision‑making.1,2 MF‑related anemia is multifactorial, with contributing mechanisms including ineffective erythropoiesis, inflammatory cytokine signaling, splenic sequestration, nutritional deficiencies, and treatment‑related myelosuppression, particularly with first-generation Janus kinase (JAK) inhibitors (Figure 1).1-3
Figure 1. Key contributors to myelofibrosis‑related anemia.*
The therapeutic landscape for MF‑associated anemia has evolved considerably in recent years with the approval of JAK inhibitors with anemia‑sparing properties and increasing integration of targeted anemia‑directed therapies.1,2,5 The 2024 British Society for Haematology (BSH), Onkopedia 2025, Grupo Español de Enfermedades Mieloproliferativas Filadelfia Negativas (GEMFIN; Spanish Group of Philadelphia-negative Myeloproliferative Neoplasms) 2025, and National Comprehensive Cancer Network (NCCN) Guidelines for Myeloproliferative Neoplasms (Version 1.2026), provide complementary, evidence‑based frameworks for managing anemia across diverse MF clinical scenarios.1,4-6 Here, we summarize and contextualize the latest recommendations, with a focus on practical treatment selection.
Anemia assessment in MF
Anemia management should begin with a systematic evaluation to confirm disease attribution and identify reversible contributors.1,4,5 Recommended baseline investigations should assess for reversible contributors to anemia, including hematinic deficiencies and hemolysis, alongside serum erythropoietin (EPO) levels and transfusion requirements.1,4,5 Bone marrow assessment and molecular profiling are integral to disease diagnosis and prognostic risk stratification in MF.1,2,5 Anemia severity is incorporated into modern prognostic models such as DIPSS-Plus, MIPSS-70, and MIPSS-70+ version 2.0, reflecting its established role as both a marker of disease biology and an independent predictor of survival.1,2,5 The NCCN guidelines further distinguish anemia management pathways based on the presence or absence of symptomatic splenomegaly and constitutional symptoms, recognizing that anemia‑directed therapy must be integrated with broader disease control strategies.1
Therapeutic management of anemia in MF
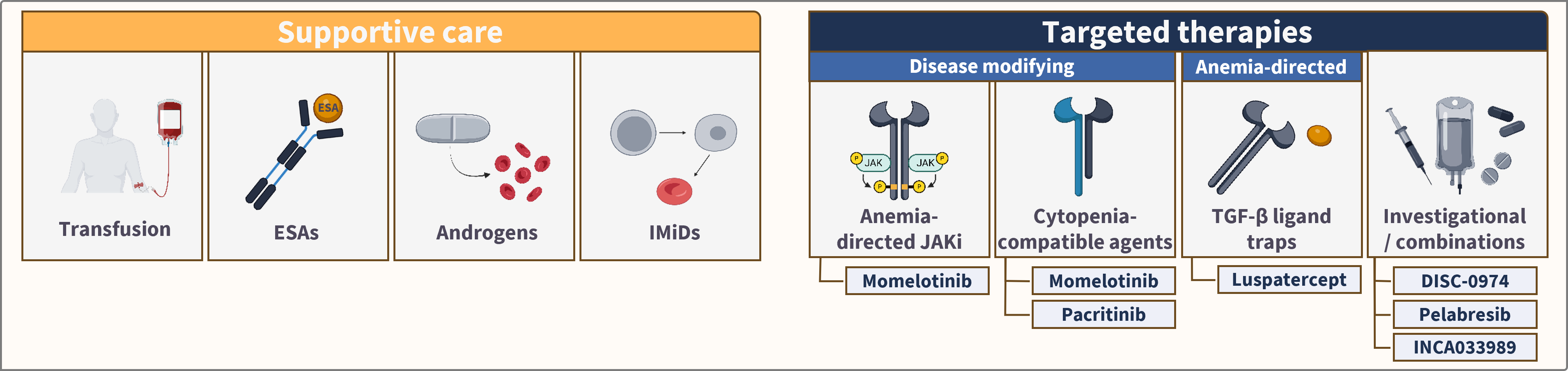
The management of cytopenic MF requires a balance of cytopenia support and disease-directed therapy (Figure 2).2,3 Traditionally, MF-related anemia has been managed with supportive therapies alongside treatment of the underlying MF; including, for example, red blood cell (RBC) transfusions, erythropoiesis-stimulating agents (ESAs), androgens such as danazol, and dose modification of JAK inhibitors where appropriate. More recently, treatment strategies have evolved toward therapies that address both the underlying disease and anemia burden.2,3 Two targeted therapies (both JAK inhibitors) are currently approved for patients with cytopenic MF: momelotinib in the US and Europe, and pacritinib in the US only.1,7 Momelotinib has a dual JAK1/2 and ACVR1 inhibition mechanism of action, and has demonstrated consistent improvements in transfusion independence observed in phase III studies.8 Pacritinib has expanded therapeutic options for patients with severe thrombocytopenia, particularly those with platelet counts <50 × 10⁹/L, in whom conventional JAK inhibitor dosing may be limited.1,4-6 Luspatercept is approved in the US for the treatment of anemia without previous use of ESAs in adults with very low- to intermediate-risk myelodysplastic syndromes (MDS) who may require regular RBC transfusions; and for the treatment of anemia refractory/intolerant to prior ESA treatment that requires ≥2 RBC transfusions over 8 weeks in adults with very low- to intermediate-risk MDS with ring sideroblasts or with myelodysplastic/MPN with ring sideroblasts and thrombocytosis.1 Although these approvals are in MDS rather than MF, luspatercept has demonstrated activity in improving anemia and reducing transfusion burden in patients with MF in clinical studies and has been included in treatment guidelines as a therapeutic option for MF-related anemia.1
Figure 2. Current therapeutic approach to cytopenic myelofibrosis2,9-12
NCCN 2026 guidelines
The NCCN 2026 guidelines dedicate a specific treatment algorithm for MF‑associated anemia (MF‑3), highlighting its clinical importance. Across all scenarios, participation in a clinical trial is listed as the preferred option when available. Outside of trials, therapeutic selection is guided by symptom burden, splenic status, serum EPO level, current JAK inhibitor therapy, and the presence or absence of constitutional symptoms.1 Momelotinib is listed as a preferred regimen in patients with anemia and ongoing symptomatic splenomegaly and/or constitutional symptoms, and as another recommended regimen in patients with no splenomegaly or significant symptoms.1 Pacritinib is also included as an alternative in these clinical scenarios.1 Other recommended regimens include JAK inhibitor combinations with anemia‑directed agents including luspatercept, ESAs, and danazol.1 Luspatercept and danazol are also listed as other recommended regimens in patients without splenomegaly or constitutional symptoms, independent of combination JAK inhibitor therapy.1 ESAs are recommended only for patients with serum EPO levels <500 mU/mL, consistent with limited efficacy in EPO‑replete disease.1 Lenalidomide plus prednisone is listed as useful in certain circumstances for patients with del(5q), reflecting modest activity and toxicity considerations.1 The NCCN guidelines distinguish patients with ongoing symptomatic splenomegaly and/or constitutional symptoms from those with adequate disease control.1 In patients whose splenomegaly and constitutional symptoms are well controlled on a JAK inhibitor, add-on anemia-directed therapy is listed as another recommended approach.1 Switching to momelotinib or pacritinib may be useful in certain circumstances (Table 1).1
Table 1. NCCN 2026 recommendations for the management of MF‑associated anemia following assessment for and treatment of alternative causes of anemia1
| Ongoing symptomatic splenomegaly and/or constitutional symptoms | No symptomatic splenomegaly or constitutional symptoms | Splenomegaly and constitutional symptoms well controlled on current JAKi | |
| Preferred regimens | Clinical trial | Clinical trial | Clinical trial |
| Momelotinib (category 1) | |||
| Other recommended regimens | Pacritinib | ESAs (if serum EPO <500 mU/mL) | JAKi in combination with ESAs (if serum EPO <500 mU/mL), luspatercept, or danazol (category 2B) |
| Ruxolitinib in combination with luspatercept or ESAs (if serum EPO <500 mU/mL; category 2B*) | Luspatercept | ||
| Danazol (category 2B) | Danazol | ||
| Pacritinib (category 2B) | |||
| Momelotinib (category 2B) | |||
| Useful in certain circumstances | — | Lenalidomide + prednisone for patients with del(5q) (category 2B) | Change to pacritinib |
| Change to momelotinib | |||
Note: All recommendations are Category 2A unless otherwise indicated. | |||
BSH 2024 guidelines
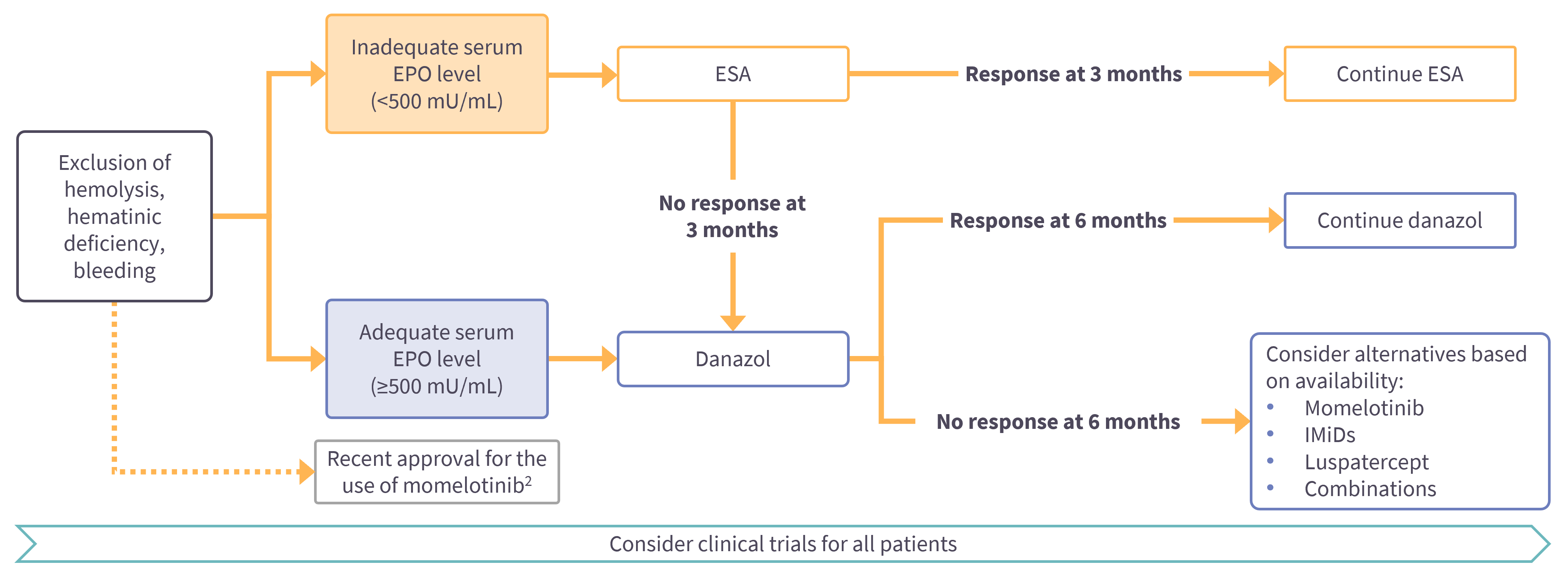
The BSH 2024 guidelines recommend ESAs for patients with anemia and inadequate EPO levels, with response rates of ~50%.4 A 12-week trial is advised, including in combination with ruxolitinib. Danazol is recommended as an initial or subsequent option, either alone or in combination with ruxolitinib, with hemoglobin responses observed in up to 30% of patients as monotherapy, and up to 55% of patients when combined with ruxolitinib.4 A minimum 3- to 6-month trial is required, with monitoring for androgen-related toxicity.4 Immunomodulatory drugs may be considered after ESA and danazol failure, although their role is limited by low overall response rates, toxicity, and access constraints in the UK.4 RBC transfusion remains the mainstay of anemia management when other measures are ineffective, with iron chelation considered in transfusion-dependent and/or iron-overloaded patients, particularly those eligible for allogeneic stem cell transplantation.4 The BSH guidelines recommend consideration of momelotinib for patients with MF and anemia irrespective of whether it is used in first-line, second-line, or later treatment settings, reflecting its ability to improve splenomegaly and symptom burden while also addressing anemia, irrespective of baseline serum EPO levels (Figure 3).4
Figure 3. BSH 2024 recommendations for the management of MF-associated anemia*
Onkopedia 2025 guidelines
Onkopedia, a German Society for Hematology and Medical Oncology (DGHO) initiative, provides evidence-based guidelines for the diagnosis and treatment of hematological and oncological diseases. The Onkopedia 2025 guidelines provide a European perspective on MF management and broadly align with the NCCN and BSH recommendations, while highlighting several additional considerations.5 Symptomatic therapy remains central to MF management, with oral JAK inhibitors forming the basis of treatment for symptomatic disease.5 Ruxolitinib has become standard therapy, with fedratinib and momelotinib available as alternative JAK inhibitors.5 The Competence Center for Oncology of the Medical Services and the Federal Institute for Drugs and Medical Devices provided guidance in 2024 on the eligibility for a JAK inhibitor as a second-line therapy.5 Based on data submitted to the European Medicines Agency, they state that, following ruxolitinib treatment, momelotinib or fedratinib should be considered; with all other combinations being off-label.5 This also applies to prior clinical trial participation and to third-line therapy.5 The guideline states that in cases of significant anemia, a lower starting dose of ruxolitinib (which can be increased over time) or primary therapy with momelotinib is recommended.5 It also highlights the role of momelotinib in patients with clinically symptomatic, moderate to severe anemia and platelet count >25 × 10⁹/L.5,7 Momelotinib has also been available for MF in the EU (regardless of risk score) since 2024 and in Switzerland (for intermediate- or high-risk scores) in cases of moderate/severe anemia or after prior ruxolitinib treatment.5 The Onkopedia guidelines also outline several problem-oriented treatment strategies for anemia, including ESAs, androgens such as danazol, RBCs, corticosteroids, and immunomodulatory drugs.5 These recommendations emphasize individualized treatment based on symptom burden, transfusion dependence, and disease risk.5,7
GEMFIN 2025 guidelines
The GEMFIN 2025 guidelines emphasize an increasingly phenotype-adapted approach to MF management, recognizing anemia and thrombocytopenia as important determinants of therapeutic selection and sequencing.6 The guidance recognizes that cytopenias frequently influence JAK inhibitor dosing, treatment selection, and long-term disease management, supporting earlier adaptation of therapy in patients with anemia and/or thrombocytopenia.6 Supportive strategies, including transfusion support, ESAs (particularly in patients with low serum EPO levels), danazol, and luspatercept for selected patients with transfusion-dependent anemia, remain important components of care.6 The guidelines highlight momelotinib as a relevant option for patients with MF-related anemia, due to its differentiated activity across anemia, symptom, and splenomegaly endpoints.6 They note that momelotinib can be administered at 200 mg/day regardless of initial platelet counts and can be considered for patients with platelet levels <50 × 10⁹/L.6 Overall, the GEMFIN guidelines support earlier therapeutic adaptation according to dominant disease phenotype and evolving clinical need, particularly in patients with anemia and thrombocytopenia.6
Areas of convergence across current guidelines
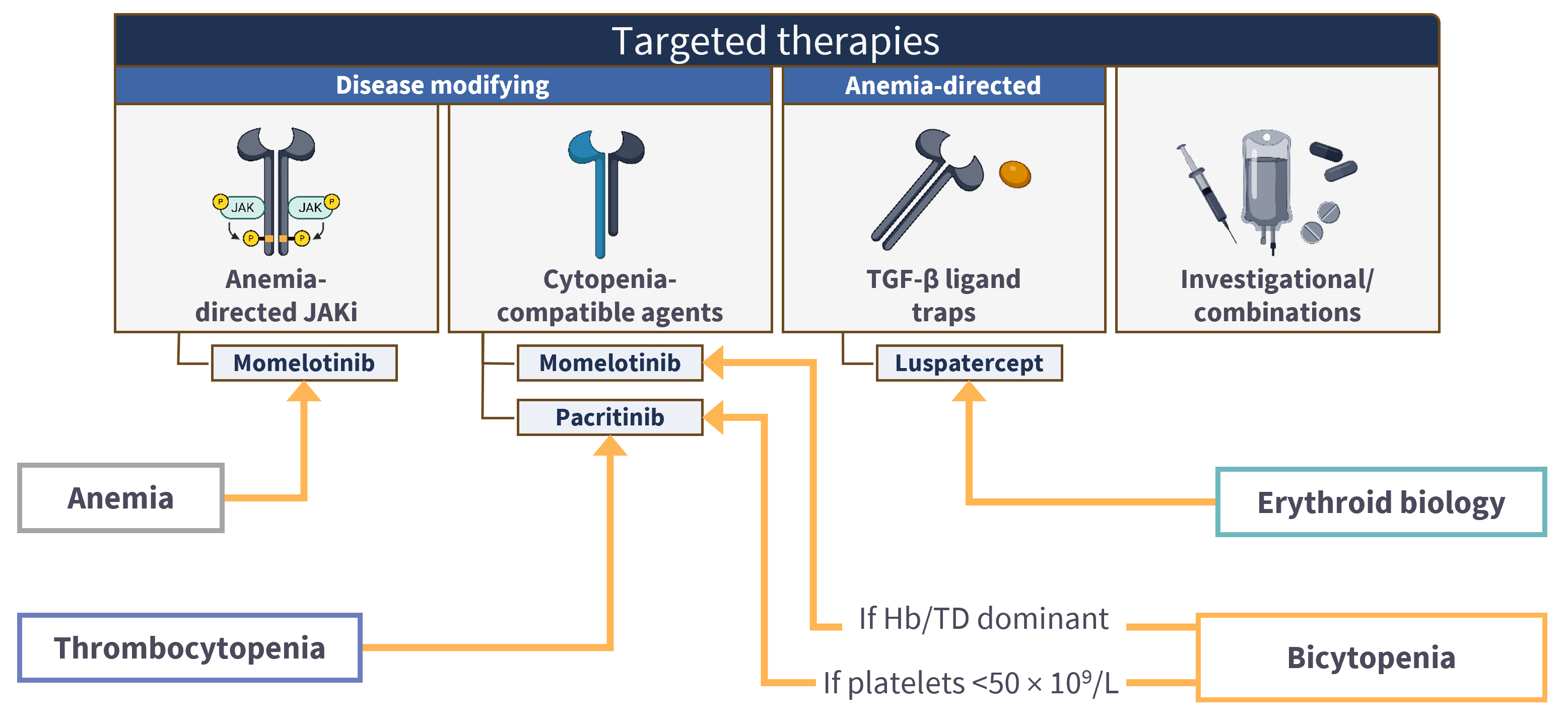
The NCCN, BSH, Onkopedia, and GEMFIN guidelines all reflect a shift in MF management from predominantly symptom- and splenomegaly-directed treatment toward a more phenotype-adapted approach incorporating anemia severity, thrombocytopenia, transfusion burden, and molecular risk stratification into therapeutic decision-making.4-6 Historically, cytopenias were frequently managed with supportive strategies, including transfusion support, ESAs, danazol, and dose modification of JAK inhibitors.1,4-6 Anemia is increasingly recognized as a major determinant of therapeutic selection, and more recent guidance has incorporated emerging anemia-directed approaches such as luspatercept in selected patients with transfusion-dependent anemia or persistent symptomatic anemia. The BSH guidelines recommend consideration of momelotinib for patients with MF and anemia, irrespective of treatment line.1,4-6 The Onkopedia guidelines similarly highlight momelotinib as being relevant for patients with clinically significant moderate-to-severe anemia.5 Pacritinib has expanded therapeutic options for patients with severe thrombocytopenia, in whom conventional JAK inhibitor dosing may be limited.1,4-6 Collectively, these recommendations support earlier treatment modification according to dominant clinical need, rather than delaying treatment modification until advanced cytopenias or treatment intolerance develop.1,4-6 While alignment on sequencing of therapies differs somewhat between guidelines and regulatory differences occur between regions, a general overview of integrating novel therapies into the clinical management of MF‑related anemia is outlined in Figure 4.1,4-6
Figure 4. Integrating novel targeted therapies into the clinical management of MF‑related anemia.1,4-6
Conclusion
The latest guidelines reflect an important shift in the management of MF‑related anemia, moving from predominantly supportive care towards mechanism‑informed, targeted therapies.1,4-6 The emergence of newer JAK inhibitors with comparatively favorable cytopenic profiles has expanded therapeutic options, enabling more integrated care.1,4-6 The optimal management of patients with MF-related anemia requires careful characterization of the underlying anemia drivers and clinical context, ongoing reassessment during therapy, and an individualized treatment approach aligned with patient‑specific goals and disease biology. 1,4-6 Ongoing clinical studies and real-world experience with novel agents and combination strategies will further inform the refinement of anemia-focused strategies for the optimal treatment of patients with MF.1,2,7
This educational resource is independently supported by GSK. All content is developed by SES in collaboration with an expert steering committee. Funders are allowed no influence.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content



