All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the MPN Advocates Network.
The MPN Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the MPN Hub cannot guarantee the accuracy of translated content. The MPN Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The MPN Hub is an independent medical education platform, sponsored by GSK, Novartis, AOP, Sobi and Takeda and supported through independent educational grants from Bristol Myers Squibb, Blueprint Medicines, Incyte and Merck Sharp & Dohme LLC, Rahway, NJ, USA. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View MPN content recommended for you
Symposium | Advanced systemic mastocytosis: Clinical challenges and unmet needs
Featured:
 Andreas Reiter
Andreas ReiterDo you know... Why may advanced systemic mastocytosis remain underrecognized in clinical practice despite established diagnostic frameworks?
At the European Hematology Association (EHA) 2026 Congress, June 11–14, 2026, Stockholm, SE, the MPN Hub held a symposium, titled Advanced systemic mastocytosis: Redefining the disease, rethinking patient outcomes. During the symposium, Andreas Reiter, University Hospital Mannheim, Mannheim, DE, delivered a presentation on clinical challenges and unmet needs in advanced systemic mastocytosis (AdvSM).
Symposium | Advanced systemic mastocytosis: Clinical challenges and unmet needs
Symposium | Advanced systemic mastocytosis: Clinical challenges and unmet needs
In this presentation, Reiter discusses how genetic complexity underpins disease heterogeneity and clinical presentation in AdvSM, how variable disease presentation can lead to diagnostic delays, and that treatment outcomes highlight variability across AdvSM subtypes. He explores the limitations of conventional disease burden assessment, the variable symptom burden impacts on quality of life (QoL) across systemic mastocytosis (SM) subtypes, and how disease heterogeneity can lead to complexity in AdvSM management. In addition, he discusses the variability in morphology and genetics in SM with an associated hematologic neoplasm (SM-AHN) and illustrates potential challenges in clinical practice using a patient case study.
Key points
- AdvSM is driven not only by KIT D816V, but by multilineage involvement and accumulation of additional somatic mutations that can influence disease behavior and prognosis.1
- ~90% of patients with AdvSM have additional somatic mutations beyond KIT D816V.1
- Multilineage mutations have been associated with significantly inferior overall survival.1
- There is variability in morphology and genetics in AdvSM, including variability in mast cell burden, KIT D816V burden, and AHN involvement, as observed in SM-chronic myelomonocytic leukemia (Figure 1).1
Figure 1. Representative patient profiles illustrate the variability in mast cell burden, KIT D816V burden, and AHN involvement observed in SM-CMML/-AML*
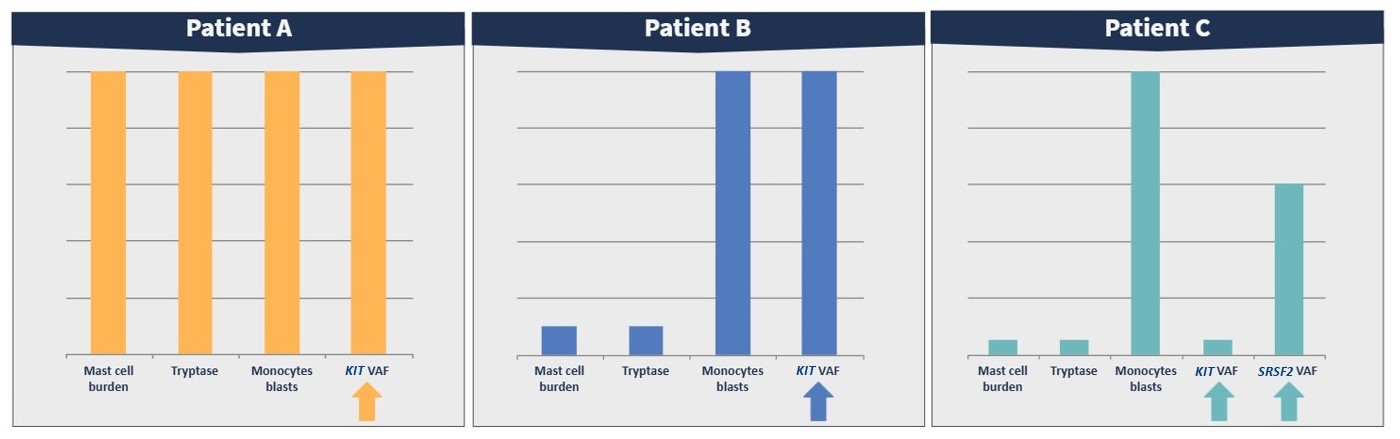
- Bone marrow mast cell infiltration and serum tryptase reflect mast cell burden but do not fully capture overall disease burden, which is also influenced by KIT D816V allele burden and additional somatic mutations.1
- Patterns of organ damage, cytopenias, and symptoms vary widely between patients with AdvSM, and this heterogeneity affects clinical presentation, diagnosis, treatment decisions, and the patient experience.1-3
- AdvSM is rare and frequently underrecognized, contributing to delayed diagnosis and missed recognition of both SM and AHN components. Variable disease presentation can contribute to diagnostic delays.2,3
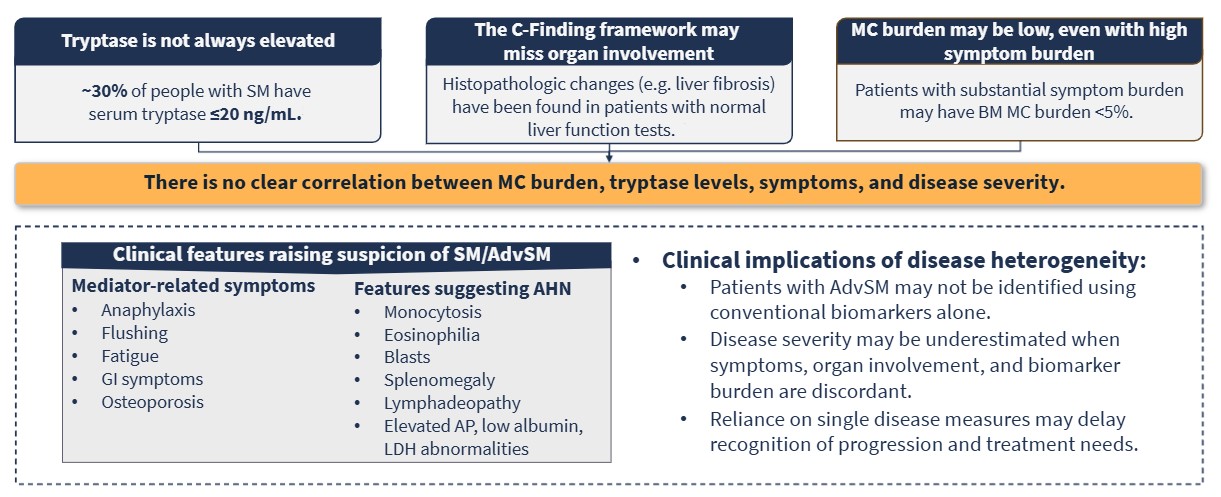
- There are limitations to conventional disease burden assessment. It cannot be fully captured by a single biomarker and requires integrated clinical and molecular assessment (Figure 2).3,4
Figure 2. Disease burden assessment requires integrated clinical and molecular assessment
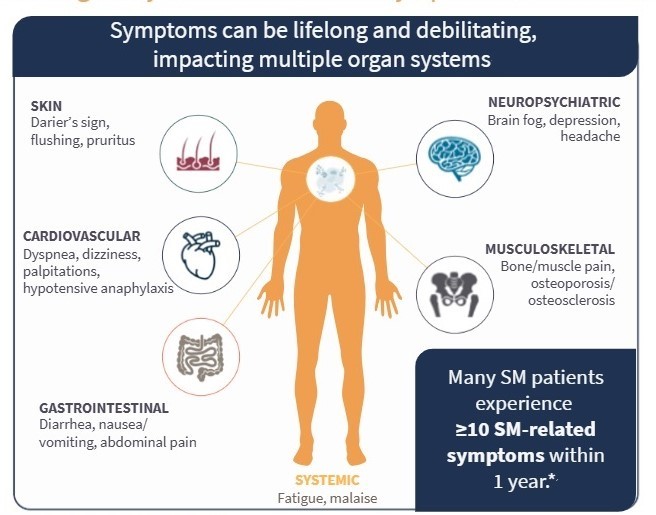
- Heterogeneity results in variable symptom burden impacts on QoL across SM subtypes, with symptom burden affecting patients across multiple domains (Figure 3).3,4
- The symptom burden impacts on QoL can be significant, with studies indicating that ~50% of patients with SM that may reduce their working hours and ~60% that may avoid leaving home because of their symptoms.3,4
Figure 3. Potential symptoms of systemic mastocytosis*
- Treatment outcomes highlight variability across AdvSM subtypes, with subtype biology underlying the wide variability in clinical outcomes.5,6
- Survival outcomes with midostaurin vary across subtypes, with the poorest outcomes in SM-AHN and mast cell leukemia.5
- Selective KIT inhibitors improve outcomes, but treatment responses are higher in treatment-naïve cohorts.5,6
- Targeted KIT inhibitors such as midostaurin and avapritinib have shifted the treatment paradigm, but gaps may remain between molecular clearance and symptom relief, timing of treatment, and sequencing. As the treatment landscape evolves, the timing of intervention may be critical.5,6
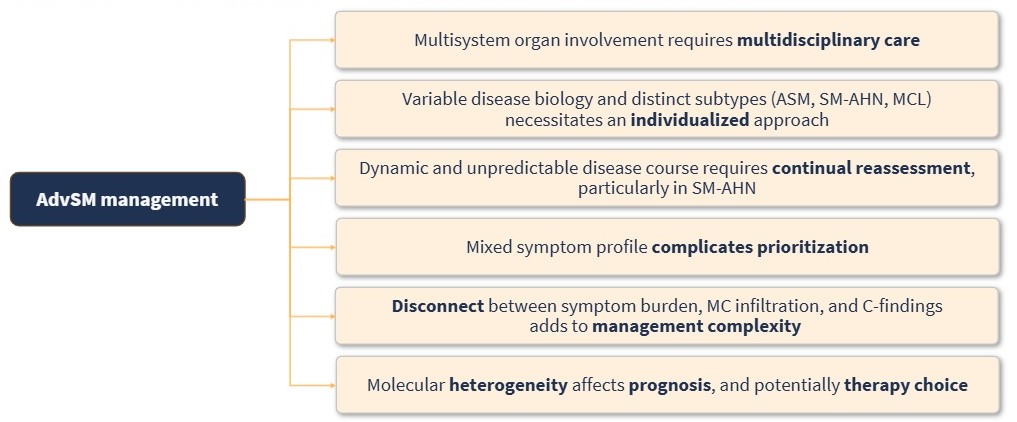
- Overall, heterogeneity leads to complexity in AdvSM management; individualized and complex management strategies are needed, which require integration of symptom control, organ-directed therapy, molecular risk stratification, and multidisciplinary care (Figure 4).1,4
Figure 4. Complexity in AdvSM management*
This educational resource is independently supported by Blueprint medicines. All content is developed by the faculty in collaboration with SES. Funders are allowed no influence.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
More from this series:




