All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the MPN Advocates Network.
The MPN Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the MPN Hub cannot guarantee the accuracy of translated content. The MPN Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The MPN Hub is an independent medical education platform, sponsored by GSK, Novartis, AOP, Sobi and Takeda and supported through independent educational grants from Bristol Myers Squibb, Blueprint Medicines, Incyte and Merck Sharp & Dohme LLC, Rahway, NJ, USA. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View MPN content recommended for you
Symposium | Cytopenias in MF: Clinical burden and the need for prioritized management
Featured:
 Jean-Jacques Kiladjian
Jean-Jacques KiladjianDo you know... Regarding the incidence of cytopenias at diagnosis in patients with myelofibrosis, which of the following statements is correct?
At the ESH 11th Translational Research Conference: Myeloproliferative Neoplasms, Apr 24–26, 2026, Estoril, PT, the MPN Hub held a symposium, titled Patient-centered approaches in myelofibrosis: Tailoring treatment for anemia and thrombocytopenia. During the symposium, MPN Hub Steering Committee Chair Jean-Jacques Kiladjian, Université Paris Cité - Hôpital Saint-Louis, Paris, FR, delivered a presentation on cytopenias in myelofibrosis (MF), with a focus on clinical burden and the need for prioritized management.
Symposium | Cytopenias in MF: Clinical burden and the need for prioritized management
Symposium | Cytopenias in MF: Clinical burden and the need for prioritized management
In this presentation, Kiladjian discusses the drivers and incidence of cytopenias in MF, transfusion burden associated with anemia, the impact of cytopenias on symptom burden and quality of life (QoL), treatment adjustments necessitated by cytopenias, and the impact of cytopenias on outcomes, highlighting that cytopenia management is central to patient-centered care in MF.
Key points
- The drivers of anemia and thrombocytopenia in MF are multifactorial (Figure 1), and the pathogenesis of anemia in MF is only partially understood.1,2
Figure 1a. Drivers of cytopenias in myelofibrosis in anemia and B thrombocytopenia*
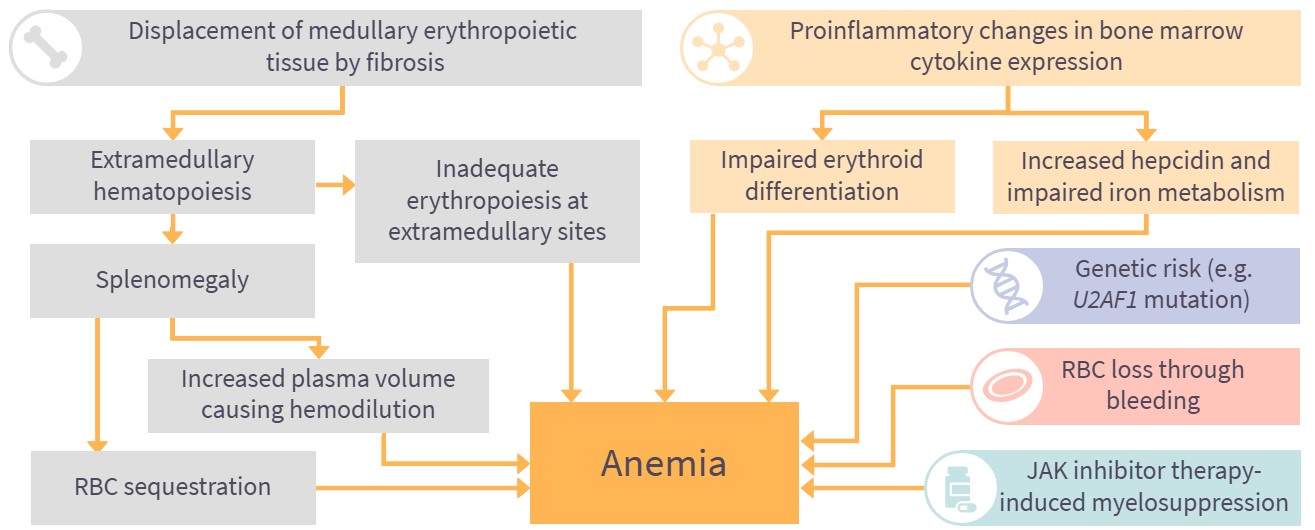
Figure 1b. Drivers of cytopenias in myelofibrosis in and thrombocytopenia*
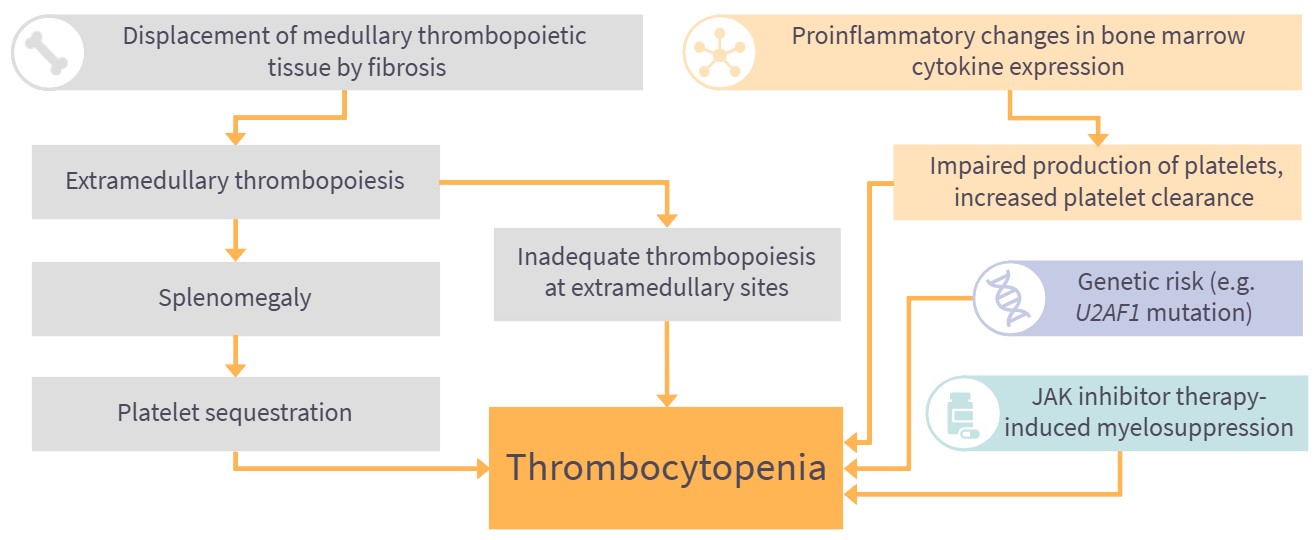
- Cytopenias are a common clinical manifestation of MF, with anemia (defined as hemoglobin <10 g/dL) present in almost 40% of all patients with MF at diagnosis and thrombocytopenia (defined as platelet count <100 × 109/L) in 16–26% of patients at diagnosis.1,2
- Anemia in MF often leads to transfusion dependence, with around a quarter of patients red blood cell (RBC)-transfusion dependent at diagnosis and most patients developing transfusion dependence over their disease course.1
- RBC transfusion-dependence is associated with poorer QoL and reduced survival compared with transfusion independence.1
- Cytopenias in MF have significant impacts on symptom burden and QoL, and these impacts increase with worsening anemia and thrombocytopenia.3–5
- Cytopenias in MF often result in treatment modifications, with anemia and thrombocytopenia among the most common reasons for dose modification.6,7
- Dose reductions and dose interruptions due to cytopenias are reported in 67.4% and 27.2% of patients with MF, respectively.6,7
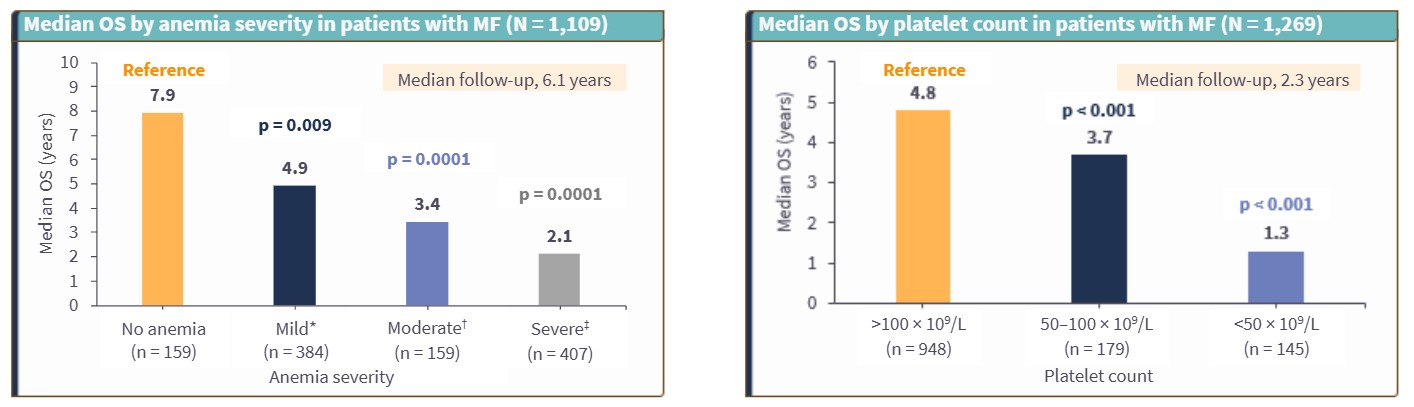
- Cytopenias are associated with reduced survival in MF, with the presence of severe anemia or transfusion dependence associated with a 1.5-fold increase in risk of death vs moderate anemia, and the presence of thrombocytopenia associated with a 1.4-fold increase in risk of death vs platelet counts >100 × 109/L (Figure 2).8,9 Increasing severity of cytopenias is associated with progressively poorer overall survival.8,9
Figure 2. Impact of cytopenias on overall survival in patients with myelofibrosis in A anemia and B thrombocytopenia*
- Cytopenia management is central to patient-centered care in MF, and treatment strategies should address cytopenias, in order to reduce transfusion dependence, improve QoL, reduce dose reductions/interruptions, and improve prognosis.1,8,9
This educational resource is independently supported by GSK. All content is developed by the faculty in collaboration with SES. Funders are allowed no influence.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
More from this series:



