All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the MPN Advocates Network.
The MPN Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the MPN Hub cannot guarantee the accuracy of translated content. The MPN Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The MPN Hub is an independent medical education platform, sponsored by GSK, Novartis, AOP, Sobi and Takeda and supported through independent educational grants from Bristol Myers Squibb, Blueprint, Incyte and Merck Sharp & Dohme LLC, Rahway, NJ, USA. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View MPN content recommended for you
Symposium | How to treat cytopenic myelofibrosis: Treatment algorithms and real‑world insights
Featured:
 Claire Harrison
Claire HarrisonDo you know... According to guideline recommendations and real-world evidence, which of the following is the most appropriate first-line treatment approach for patients with myelofibrosis and symptomatic anemia with a platelet count >100 × 10⁹/L?
At the ESH 11th Translational Research Conference: Myeloproliferative Neoplasms, April 24–26, 2026, Estoril, PT, the MPN Hub held a symposium, titled Patient-centered approaches in myelofibrosis: Tailoring treatment for anemia and thrombocytopenia. During the symposium, MPN Hub Steering Committee member Claire Harrison, Guy's and St Thomas' NHS Foundation Trust, London, UK, delivered a presentation on treatment options for patients with cytopenic myelofibrosis (MF), reviewing treatment algorithms and providing real‑world insights.
Symposium | How to treat cytopenic myelofibrosis: Treatment algorithms and real‑world insights
Symposium | How to treat cytopenic myelofibrosis: Treatment algorithms and real‑world insights
In this presentation, Harrison discusses the impact of transfusions on patients with MF and MF subgroups, as well as the British Society for Haematology (BSH) 2024 and National Comprehensive Cancer Network (NCCN) 2026 guidelines for managing cytopenias in patients with MF. She also reviews real-world evidence for current treatment options, using patient cases to illustrate treatment selection in the clinical setting.
Key points
- The impact of transfusions on patients with MF is pronounced, with transfusion-dependent (TD) patients rating their hospital experience as worse than transfusion-independent patients, and reporting greater impacts on their work, social, and daily lives.1
- Improving anemia and reducing transfusion frequency are considered important treatment goals for ~80% of patients with anemic MF.2
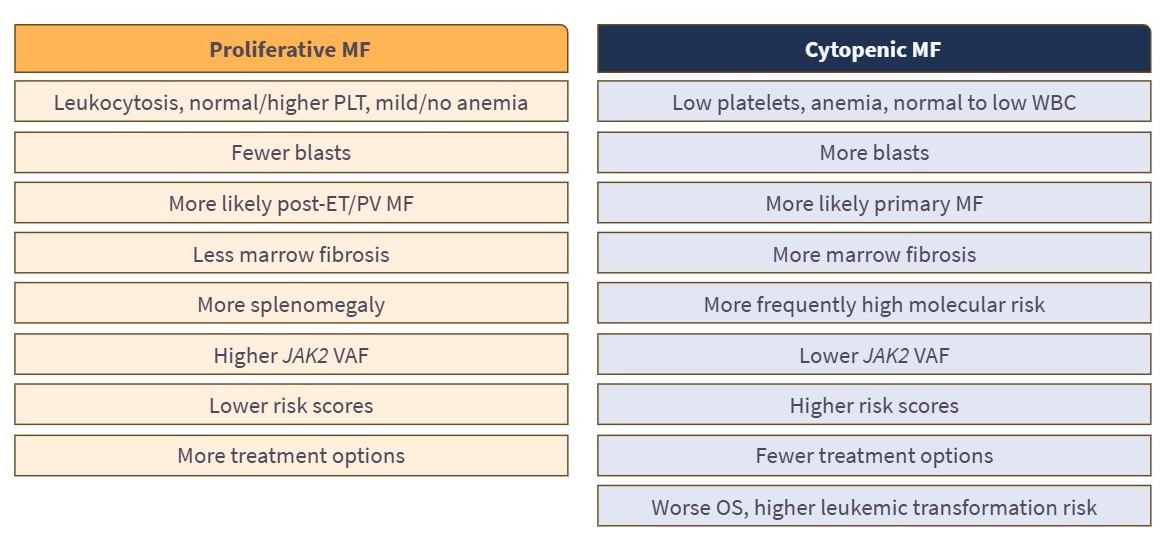
- The characteristics of proliferative vs cytopenic MF are outlined in Figure 1.
Figure 1. MF subgroups: Proliferative vs cytopenic*
- The BSH 2024 guidelines provide a suggested algorithm for managing anemia in patients with MF, highlighting that clinical trials should be considered for all patients. They also note that momelotinib, immunomodulatory drugs (IMiDs), luspatercept, and combination therapies can be considered as alternative treatments for managing anemia in MF if there is no response to erythropoiesis-stimulating agents (ESAs) or danazol by 3 and 6 months, respectively (Figure 2A).4
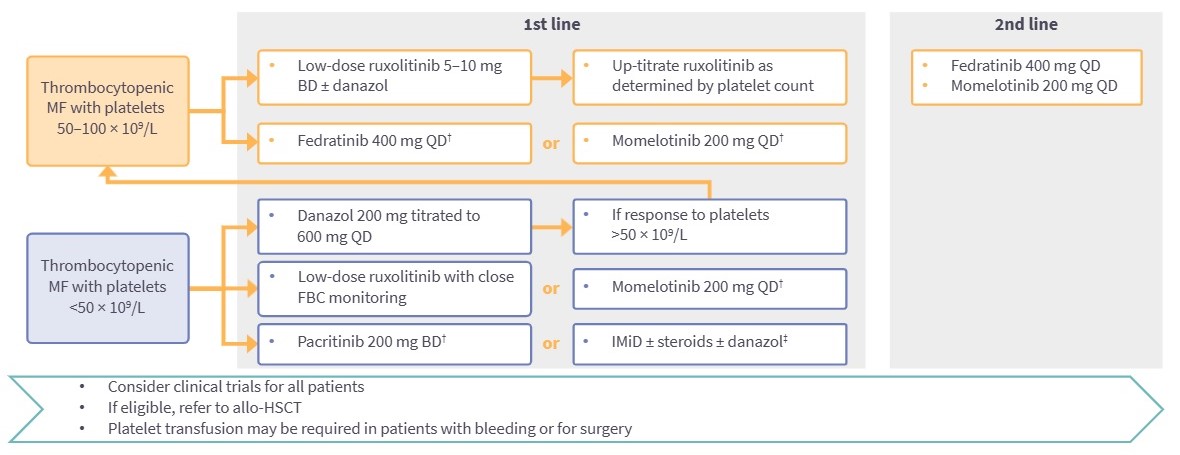
- The BSH guidelines also provide a potential algorithm for the management of patients with MF and thrombocytopenia, highlighting platelet count-guided use of low-dose ruxolitinib (with or without danazol), fedratinib, momelotinib, pacritinib, and supportive approaches such as danazol or IMiD-based therapy, with escalation to standard Janus kinase inhibitor (JAKi) dosing where platelet counts improve and consideration of fedratinib or momelotinib as second-line options (Figure 2B).4
Figure 2A. BSH 2024 guidelines: Suggested algorithm for managing anemia in patients with MF*
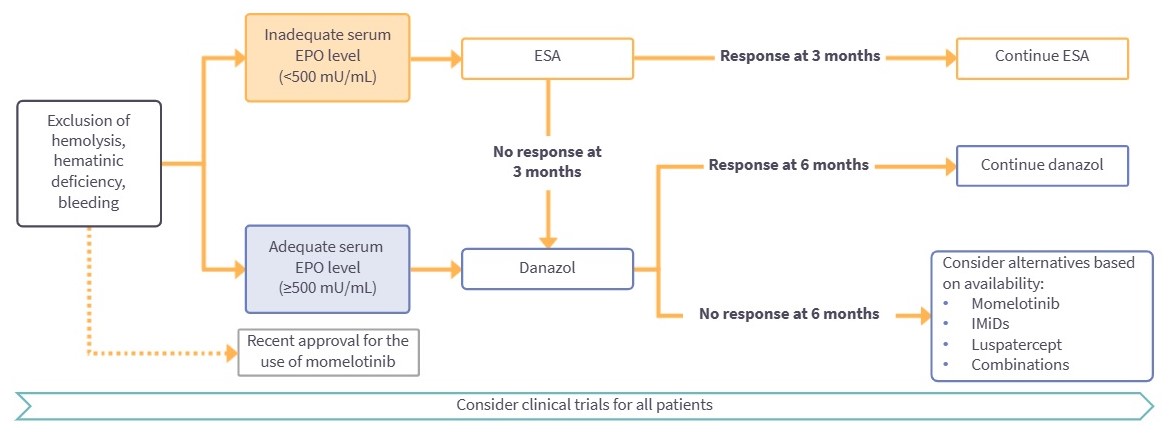
Figure 2B. BSH 2024 guidelines: Potential algorithm for the management of patients with MF and thrombocytopenia*
- The NCCN 2026 guidelines concur with the recommendation of considering clinical trials for all patients and highlight the selection of momelotinib, pacritinib, ESAs, luspatercept, danazol, and combination JAKi-based strategies according to the presence of splenomegaly or constitutional symptoms, serum erythropoietin level, and response to ongoing JAKi therapy.5
- Results from MOMGEMFIN, a real-world retrospective analysis evaluating the efficacy and safety of momelotinib in patients with MF and TD anemia (n = 90), demonstrated an anemia response in 61.2% of patients and an improved symptom response in 92% of patients with disease-related symptoms at baseline (n = 134).6
- Among patients with TD anemia, 48.4% achieved transfusion independence at 3 months and 45.7% achieved transfusion independence at 6 months.6
- While thrombocytopenia was the most common hematologic adverse event (10.3% of patients), median platelet counts remained stable at 3, 6, and 9 months of treatment, including in patients with platelet counts <100 × 109/L and <50 × 109/L.6
- In a real-world retrospective analysis of luspatercept treatment in patients with MF and TD anemia, luspatercept demonstrated meaningful improvements in transfusion independence and transfusion burden in both transfusion-requiring and TD populations.6
- Pacritinib demonstrated improvements in anemia and thrombocytopenia in a real-world retrospective analysis in patients with MF, with a 6-month overall survival (OS) rate of 92% and a 30.4% platelet response rate at any time during follow-up.7
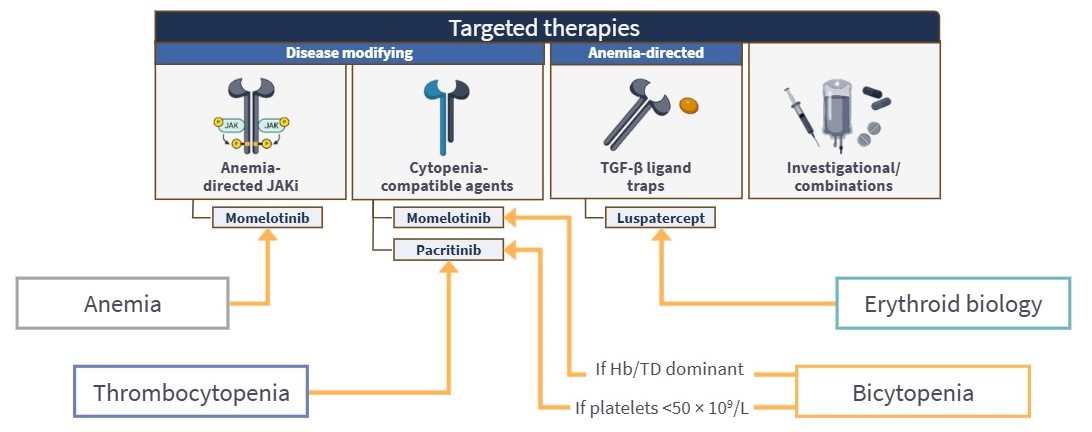
- Real-world evidence supports phenotype-driven treatment selection in patients with MF and cytopenias (Figure 3).4-7
Figure 3. Phenotype-driven treatment selection in patients with cytopenic myelofibrosis*
This educational resource is independently supported by GSK. All content is developed by the faculty in collaboration with SES. Funders are allowed no influence.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content
More from this series:



